




















Automated peritoneal dialysis (APD) with sleep•safe harmony and SILENCIA

Peritoneal Dialysis (PD) is a patient-centric therapy. Patient-centric approaches have been shown to empower patients, enhance their well-being, improve the quality of care, and add to health systems’ sustainability.1 In 2020 world-wide around 413,000 patients suffering from End Stage Kidney Disease were treated with Peritoneal Dialysis (PD) with increasing numbers.2
In the area of Continuous Ambulatory Peritoneal dialysis (CAPD) our individual clinical solutions are designed for tailoring your patients’ therapy. The CAPD treatment stay•safe system contains the safety features DISC and PIN, which are connected with the PD fluids. The stay•safe system – small details that make a big difference.
In a small usability study from Reitz et al. the sleep•safe harmony cycler demonstrated good learnability and ease of use.9
Adapted APD (aAPD) therapy with sleep•safe harmony enables you to combine sequences of short dwells and small fill volumes with long dwells and large fill volumes and varying glucose concentrations. This way of prescribing PD, proposed by Fischbach et al., may have the potential to improve ultrafiltration (UF) and clearance within one PD session.10
sleep•safe harmony offers:
We support you with a range of specific trainings that lay the foundation for a confident start to therapy. And while everybody is preparing, we help to make sure that everything is up and running in your patients’ homes.
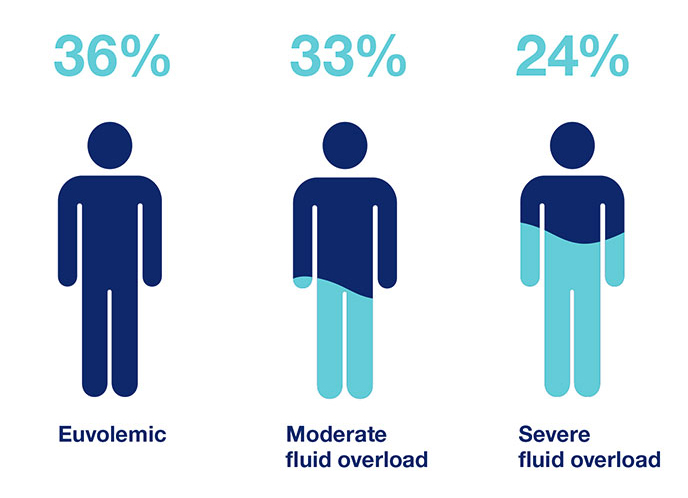
One of the major problems in today’s practice of renal replacement therapy is the quantitative assessment and management of fluid status. There are many factors known to affect fluid status such as comorbid conditions, medication, nutrition and treatment modalities.13,14
The treatment of fluid imbalance in dialysis patients is important because of its role in the development of cardiovascular (CV) diseases, which represent the leading cause of death in dialysis patients.15 Achieving euvolemia is hence a major goal in PD as both dehydration and overhydration can increase mortality through cardiovascular risk and impairment of residual kidney function (RRF).14,16
Important factors to consider in fluid status:
ISPD guidelines suggest that clinical assessment should include a diverse spectrum of clinical and laboratory results, including peritoneal and renal clearances, hydration status, appetite and nutritional status, energy level, hemoglobin concentration, responsiveness to erythropoietin therapy, electrolytes and acid–base balance, calcium phosphate homeostasis, and blood pressure control (Evidence level C).19
Fluid overload is triggered by the expansion of the extracellular water. When examining fluid overload, it is important to divide total body water (TBW) into intracellular (ICW) and extracellular water (ECW). The latter is further divided into circulating and interstitial compartments.20,21
Fluid management in peritoneal dialysis (PD) patients is highly important because it has been shown that:
This step-by-step approach is designed to support your PD patients. Based on our experience and diverse portfolio, we provide solutions for every step of fluid management. Our products and services cover the entire process and offer the chance for improved patient outcome.
The three steps consist of:
Obtain a better understanding of actual fluid status and trend
| Dehydration | Normohydration | Overhydration |
|---|---|---|
| Hypotension | Normotension | Hypertension |
| Loss of RRF | Preservation of RRF / Reduction of CV risk | Loss of RRF / LVH |
| Increased mortality | Improved survival | Increased mortality |
Volume status improvement as a result of awareness
Use the awareness for better intake control
Preserve Residual Kidney Function (RKF) longer and use the adapted PD prescription concept
The contribution of the kidney
The decline of RKF impacts clinical outcomes. Loss of RKF not only triggers fluid overload, but also contributes to inflammation, anemia, malnutrition, LVH, hypertension and cardiovascular disease.28
The contribution of the technique
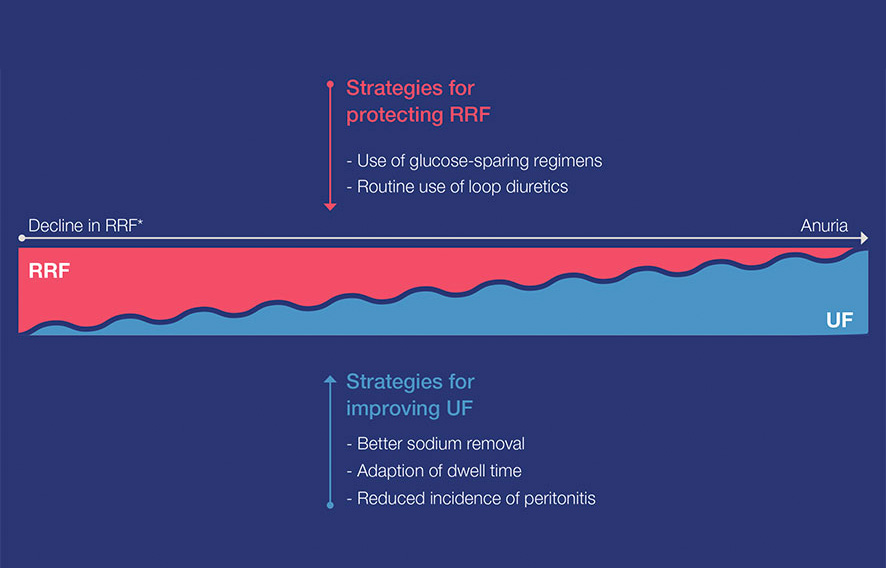
With the decrease of RKF in chronic kidney disease, ultrafiltration (UF) via PD becomes more important and challenging. PD allows an individualized dialysis prescription by combining different techniques, dialysis solutions and number and duration of dwells.17
In view of the importance of RKF and UF for successful fluid management, clinical strategies to preserving RKF and to improve UF are of paramount importance.
RKF is important for fluid and solute removal. Maintaining RKF is important for urine output and regulation of fluid status, thus using PD fluids may be an important contributor to your patient's fluid management.29
According to guidelines, it is recommended to use PD fluids that help to reduce the deleterious effects of chronic exposure to the peritoneal membrane and to preserve the membrane function longer.30,31,32
Important factors to consider in fluid status:
1 European Commission, Communication from the Commission to the European Parliament, The Council, The European Economic and Social Committee and the Committee of the Regions on enabling the digital transformation of health and care in the Digital Single Market 2018
2 Fresenius Medical Care, Annual Report 2020
3 Chan CT et al. Am J Kidney Dis 2019; 73(3):363-371
4 Auguste BL et al. Can J Kidney Health Dis 2019
5 Suri RS et al. Kidney Int. 2015; 88(2):360-8
6 Argilés A et al. Nephrology Dialysis Transplantation 2020; 35(11):1863-1839
7 Kumar VA et al. Kidney Int 2014; 86(5):1016-1022
8 Fresenius Medical Care, www.freseniusmedicalcare.asia/en/healthcare-professionals/home-therapies/staysafe-and-biofine/; 03/2022
9 Reitz T et al. Renal Replacement Therapy 2021; 7(20)
10 Fischbach M et al. Perit Dial Int 2011; 31(4):450-458
11 Vera M et al. PLoS One 2021; 16(12)
12 Punzalan S et al. Journal of Kidney Care 2017; 2(5):262-267
13 Ronco C et al. Contrib Nephrol 2012;178:164-168
14 Yong-Lim K et al. Seminars in Nephrol 2017; 37(1):43-53
15 Shu Y et al. Blood Purif 2018; 46(4):350-358
16 Jotterand Drepper V et al. PLoS One 2016; 11(7):e0158741
17 Van Biesen W et al. Clin J Am Soc Nephrol 2019; 14(6): 882-893
18 Ronco C et al. Nephrol Dial Transplant 2015; 30(5):849-858
19 Lo Wk et al. Perit Dial Int 2006; 26(5):520-522
20 Kim YL et al. Semin Nephrol 2017; 37(1):43-53
21 Chan et al. Eur J Comp Anim Pract 2014; 24:14-23
22 Cader RA et al. J Clin Nurs 2013; 22:741-748
23 Wang AY et al. Perit Dialysis Int 2015; 35:379-387
24 Luo YJ et al. Blood Purif 2011; 31:296-302
25 Wilson J et al. Semin Dial 2014; 17(4):260-4
26 Ahmad S et al. Semin Dial 2004; 17(4):284-7
27 Griva K et al. PLoS One 2014; 25;9(2):e8900
28 Marron B et al. Kidney Int Suppl 2008; 108:42-51
29 Xin L et al. Center for Kidney Diseases Nanjing Medical University 2016
30 Williams JD et al. Kidney Int 2004; 66(1):408-18
31 Weiss L et al. Perit Dial Int 2009; 29(6):630-633
32 Rippe B et al. Kidney Int 2001; 59(1):348-57
