

More care. Less complexity.
One important goal in dialysis therapy is to keep interdialytic dietary salt intake and intradialytic sodium removal balanced. Sodium load during dialysis may lead to an increase in interdialytic weight gain and hypertension, both of which are major cardiovascular risk factors.
Guidelines strongly recommend an individualized dialysate sodium4,5
The 6008 CAREsystem Sodium Management facilitates individualized dialysate sodium prescription management in order to better meet guideline recommendations. The individualized Sodium Management helps to avoid sodium load during dialysis.
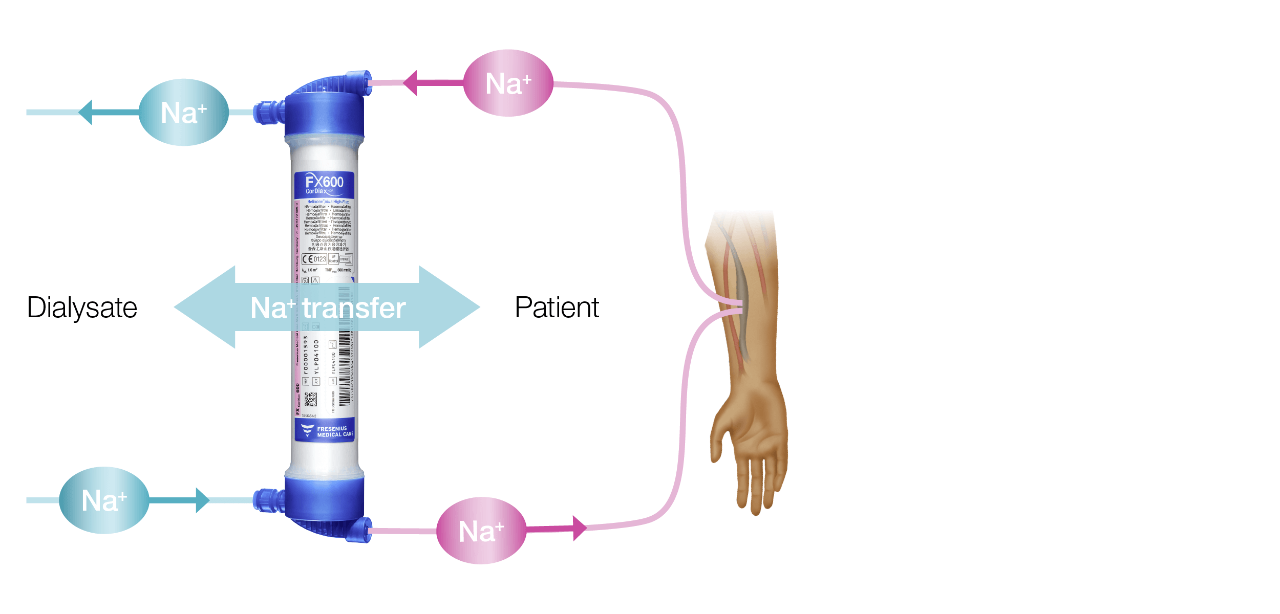
Continuous measurements of dialysate conductivity determine the amount of diffusive sodium supplied to or removed from the patient. The device continuously measures the conductivity of the incoming and outgoing dialysate and determines the sodium balance using a kinetic model. Sodium Control (Na-control) automatically adapts the dialysate sodium to the plasma sodium of the patient. It individualizes the sodium prescription, helping to avoid additional costs and workload, can make extra time-consuming blood samples obsolete and is easily implemented in clinical practice.
Salt intake during the interdialytic period is dependent on patient behavior and is a strong driver of volume overload.7 Visualization of patients’ sodium removal with Sodium Management provides information about interdialytic salt intake, enhances nutritional education and may improve HD patient outcomes.
Combining Sodium Management and BCM-based assessment of fluid status lays the path for precise and personalized sodium and fluid management and may improve hemodialysis patient outcomes.
The monitoring of predialysis plasma sodium trend data (supported by a TDMS – Therapy Data Management System**) could indicate potential pathologic changes over time.
This information may be clinically used as a trigger for further considerations in case of deviations from the normal range, or for monitoring short- and mid-term trends for potential indication of pathological changes.8
**Therapy Data Management System is an umbrella term for different products, which are optional and must be purchased separately
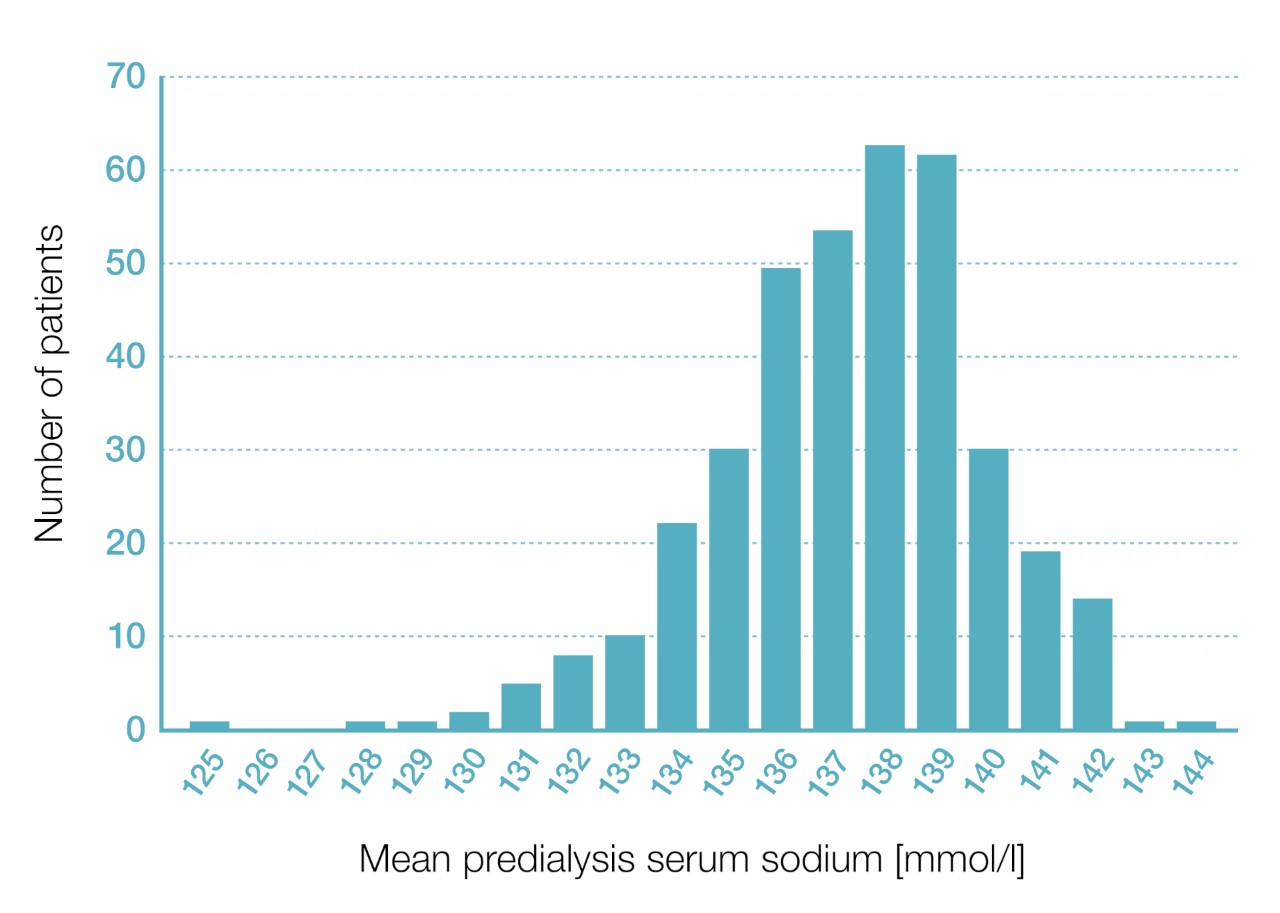
Graph: Zero sodium diffusion narrows the distribution of plasma sodium changes.9
Frequency distribution of intradialytic plasma sodium changes when dialyzing 30 patients either with a standard fixed dialysate sodium of 138 mmol/l (light blue) or with Sodium Management and a target of zero diffusive transfer (dark blue).
1.Lindley EJ, Reducing sodium intake in hemodialysis patients. Semin Dial. 2009 May-Jun;22(3):260-263.
2. Raimann JG, Thijssen S, Usvyat LA, et al., Sodium alignment in clinical practiceimplementation and implications. Semin Dial. 2011;24:587–592.
3. Sagova et al., Automated individualization of dialysate sodium concentration reduces intradialytic plasma sodium changes in hemodialysis. Artif Organs. 2019 Oct; 43(10):1002-1013.
4. National Kidney Foundation, KDOQI clinical practice guideline for hemodialysis adequacy: 2015 update. Am J Kidney Dis. 2015;66(5):884-930.
5. Kooman et al., EBPG guideline on haemodynamic instability Nephrol Dial Transplant 2007; 22 [Suppl 2]:ii22-ii44.
6. Canaud B et al., Sodium and water handling during hemodialysis: new pathophysiologic insights and management approaches for improving outcomes in end-stage kidney disease. Kidney International 2019;95:304.
7. Basile C, and Lomonte C., A neglected issue in dialysis practice: haemodialysate. Clin Kidney J. 2015;8:393–399.
8. Maierhofer A et al., EDTA-Poster 2019 FP546, “Conductivity based online estimation of predialytic plasma Na: clinical assessment”. https://academic.oup.com/ndt/article/34/Supplement_1/gfz106.FP546/5515421
9. Canaud et al., Kidney International (2019) 95, 296-309.